
As part of a research project supported by the CUNY Adjunct Incubator, Graduate Center PhD candidate Angelika Winner outlines the thinking and methods behind her ethnographic study of food provisioning practices in Newark, NJ. Taking a critical approach to the dominant narrative that links the notion of food deserts with obesity rates, Winner seeks to develop an intersectional and dynamic understanding of food environments, eating habits, access, and their entanglements with food inequities.
A Mixed Methods Study on the Relationship between Food Practices, Health Status, Social Identities, and Place of Residency
Angelika Winner
You may have heard the term food desert – a concept popular with media, government officials, and food activists alike to describe neighborhoods where residents lack physical and economic access to whole foods. Another term de jour is the so-called obesity epidemic which refers to the steep increase in overweight and obesity rates in the United States during the last few decades. Empirical evidence shows that in the US context poor and working-class populations as well as minority groups are more likely to reside in a food deserts and are also more likely to be obese or live with diet-related diseases such as diabetes and hypertension compared to wealthier and white populations. Conventionally, food deserts and the obesity epidemic are connected by a cause-and-effect relationship. In this food-desert-obesity-epidemic narrative, low-income communities and communities of color suffer from higher rates of obesity and diet-related diseases because their communities lack full-sized supermarkets. Supermarkets are assumed to provide healthier food options because they can offer better deals on produce and other healthy food products. The solution to diet-related health inequities then seems rather simple: attracting supermarkets to open stores in underserved low-income and minority communities will lead to lower rates of obesity and diet-related diseases among the residents.
However, there are several ethical as well as intellectual issues with the conventional food-desert-obesity- epidemic narrative. It can be quite rightfully argued that this narrative constitutes a form of victim blaming since the explanations for the experienced health inequities, the lack of supermarkets, are placed within the affected communities while at the same time ignoring other, external structural factors contributing to health inequities. Examples for such structural factors include class- and race-based economic inequality, residential segregation, redlining, an inadequate social safety net, and agricultural and food policies promoting energy-dense but nutrient-poor processed foods. Equally problematic are the assumptions built into the concept of food deserts, regarding the shopping behavior and store choices of people residing in food deserts. It is assumed that residents of food deserts only shop in their immediate neighborhood and, consequently, that place of residency is the most important constraining factor affecting people’s shopping behavior and store choices. It is also assumed that chain supermarkets are the only source of healthy foods, when in fact they carry plenty of processed foods. On the other hand, there are smaller independent grocers that offer many more healthy food items than chain supermarkets but are usually not considered healthy food sources in the conventional food-desert-obesity-epidemic narrative. Finally, it is assumed that low-income and minority residents in food deserts are more likely to be affected by diet-related diseases than those residents who don’t reside in food deserts, but we do not have any empirical evidence confirming this.

Ultimately, the food-desert-obesity-epidemic narrative reduces the complex issue of food justice and diet-related health inequities to a mere food supply problem. It is assumed that if the affected communities had access to supermarkets, the experienced inequities would simply go away. However, there is no scientific evidence that this is the case – the few studies that tested the effects of a new supermarket in previously underserved communities found no evidence that the diet-related health of residents improved. If we truly want to resolve diet-related health inequities, what is needed is qualitative primary data about the way people shop and the factors that constrain their shopping and store choices. We also need more detailed and more up-to-date data about food store locations, their inventories, prices, and store services. Finally, external structural factors that created health inequities and food deserts need to be considered as well. With my dissertation, I am trying to develop a less reductionist and more realistic understanding of food provisioning that moves beyond the supply-centered concept of food deserts, by investigating how people experience and navigate their food environment. I will contribute qualitative data about food stores, food and shopping practices, as well as diet-related health statuses of people with differential access to food stores in Newark, NJ.
My research is based on a mixed methods design – I am combining ethnographic methods with quantitative spatial analysis in a Geographic Information System (GIS). The two components are complementary to each other, as the quantitative spatial analysis is needed to determine which areas in Newark can be defined as food deserts, whereas the qualitative methods are needed to get at factors affecting food shopping behavior and store choice as well as diet-related health inequities. Furthermore, combining quantitative GIS-based analyses with qualitative ethnographic methods will enable me to detect where food deserts are located within the urban landscape in Newark and if their relative location affects the shopping practices and strategies of the resident people. This will also allow me to determine where people with low access to healthy food live in Newark and to compare demographic and socio-economic characteristics of areas with differential food access. To detect where food deserts are located, I am utilizing a so-called network analysis, which takes into consideration the actual walkable street distance from the spatial center of census statistical areas to the nearest supermarket qualifying as a healthy food source. The network analysis defines low-income areas that are more than a walkable distance from a supermarket as food deserts.
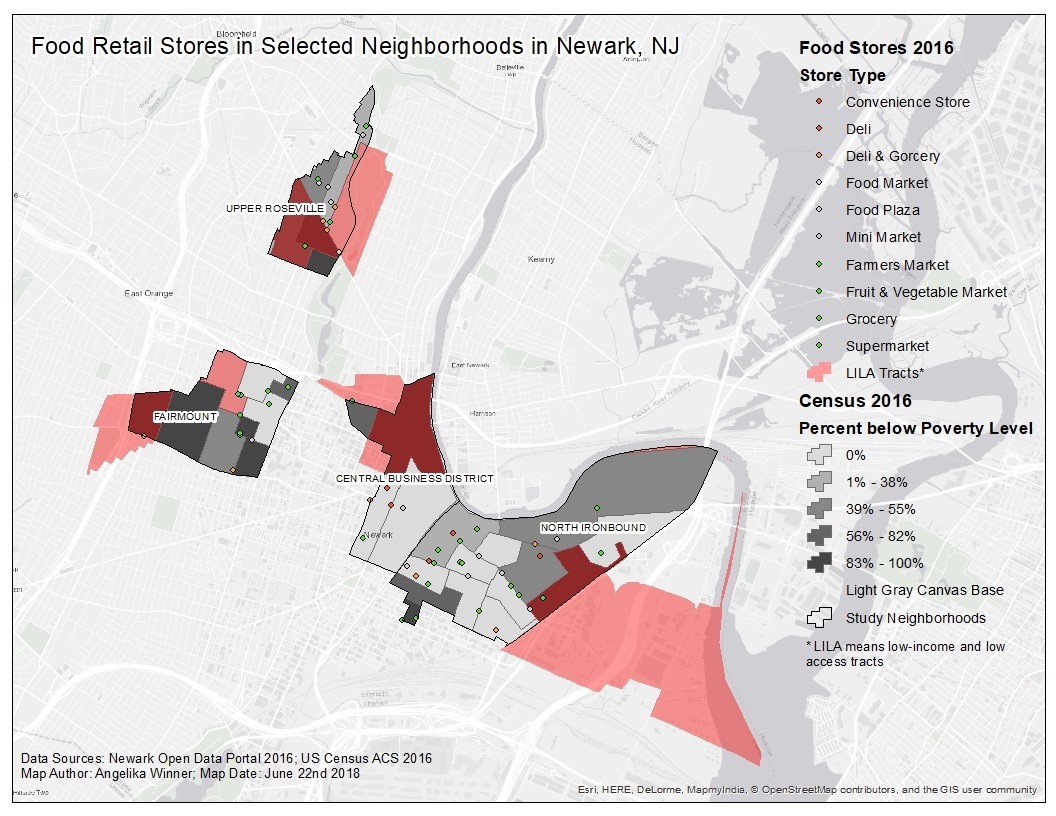
The ethnographic research component of my project has a two-legged design: I am first qualitatively observing and describing the food environment in four selected neighborhoods in Newark with the help of community volunteers, and then I am going to interview residents of Newark about their shopping and food provisioning practices and store choices with the help of food shopping diaries. For the qualitative observations, we are taking a survey of each food store (excluding restaurants and take-out places) in the selected neighborhoods, which each contain areas qualifying as food deserts, recording inventory of healthy food items (e.g. fresh produce and fruit, low-fat milk, water), prices for the recorded healthy food items, and store services (i.e. SNAP participation, deli counter, butcher/fish counter) as well as advertisement. I want to compare inventory, prices, and store services across the four neighborhoods to see if there are any differences between these variables inside and outside of food deserts. I will be interviewing people who reside in food deserts and outside of food deserts about their daily food provisioning practices, while also documenting their class, race, and gender. This will allow me to investigate if there are any differences in shopping strategies and behaviors based on the location of residence as well as based on social and cultural identities of my participants. The interviews will be conducted with the help of food shopping diaries – a qualitative method in which participants collect all receipts related to food shopping over a specified time-period (one-and-a-half-weeks in this case). In the interviews, I also want to find out what types of tensions and contradictions people experience while navigating their food environment – this includes but is not limited to economic constraints, health issues, and personal/cultural preferences.
During any ethnographic work the researcher must be sensitive to the needs and demands of the specific community one is working with. It is thus important to work closely with community members throughout the project. For my ethnographic work, I am hoping to partner with a Newark-based community group originating from the Ironbound neighborhood called Ironbound Community Corporation (ICC) which would help me to connect with local residents. ICC offers many social services to low-income residents through its community centers and offices in Newark, including food justice projects such as several urban farms and farm stands. I believe ICC will be interested in my project because the qualitative data I will collect may support new food justice policy proposals as well as their already existing food projects. ICC’s connections with local residents will be crucial for me. The partnership with ICC could provide me with the opportunity to connect with potential participants in the interviews and community volunteers that are interested in helping with data collection. I will offer to design and conduct a series of workshops for ICC about GIS technology to exchange knowledge and to enhance the toolbox of ICC to fight for social, economic, and racial justice in Newark.
In my ethnographic work I also must be sensitive to the social identities of my participants since eating and preparing food is an integral part of the formation of social identities based on gender, class, and race. Thus, feminist theories of knowledge and identity formation, namely situated knowledge and intersectionality, have been providing a useful theoretical foundation for my research, and have helped me think though my own subjectivities when it comes to food provisioning. Working from a perspective that all knowledge is situated and partial will allow me, on the one hand, to recognize my subjectivity and bias as a researcher and, on the other hand, to acknowledge and learn from “other” knowledges based on people’s experiences and lives. This means that I will carefully consider my own subjectivity and positionality. Furthermore, an ethnographic project based on the concept of intersectionality recognizes that it is neither possible to separate class from race and gender identities nor able to explain social, racial, and economic inequalities through a single framework. If social relations are reduced to just one category such as class, gender, race, or sexuality, the resulting explanations will always be partial.